Conscious Awareness & The Unconscious Mind
![]()
Whereas the brainstem mediates the more reflexive and rudimentary
aspects of vegetative and motor functioning including breathing, heart
rate, the sleep-wake cycle and arousal, the limbic system and each half of
the brain have developed their own unique strategies for perceiving,
processing, and expressing information, as well as specialized
neuroanatomical interconnections that assist in mediating these functions
(Joseph, 1982, 1986b, 1988ab, 1992ab, 1998, 2000, 2001). In humans, the
neocortical mantle of the right and left hemisphere have come to subserve
conscious awareness, including those aspects of consciousness associated
with language and thought, and those components of non-verbal and social
emotional intuitive awareness associated with the unconscious mind. By
contrast, and as is the case with all "higher" animals, the limbic system
mediates the more unconscious aspects of social-emotional and personal
awareness, including those aspects of psychic functioning associated with
what Jung referred to as the collective unconscious.
Hence, the mind and brain are hierarchically organized, the limbic
system situated above the brainstem, and the cerebral hemispheres being
organized such that two potentially independent mental systems coexist,
literally side by side.
LEFT HEMISPHERE OVERVIEW: Language & Consciousness
As is now well established, the expressive and receptive aspects of speech and language, linguistic and verbal thought, mathematical and analytical reasoning, as well as the temporal-sequential and rhythmical aspects of consciousness, are associated with the functional integrity of the left half of the brain in the majority of the population.
The left cerebral hemisphere is associated with the organization and categorization of information into discrete temporal units, the sequential control of finger, hand, arm, gestural, and articulatory movements (Beaumont 1974; Corina, et al. 1992; Haaland & Harrington, 1994; Heilman et al. 1983; Kimura 1977, 1993; Mateer 1983; McDonald et al. 1994; Wang & Goodglass, 1992) and the perception rhythm (Evers et al., 1999) and the labeling of material that can be coded linguistically or within a linear and sequential time frame (Efron, 1963; Lenneberg, 1967; Mills & Rollman, 1980). It is also dominant in regard to most aspects of expressive and receptive linguistic functioning (Evers et al., 1999; Frost, et al., 1999; Heiss, et al., 1999; Pujol, et al., 1999) including grammar, syntax, reading, writing, speaking, spelling, naming, verbal comprehension, and verbal memory. In addition, the left hemisphere has been shown via dichtoic listening tasks, to be dominant for the perception of real words, backwards speech, and consonants, as well as real and nonsense syllables (Blumstein & Cooper, 1974; Kimura, 1961; Shankweiler & Studdert-Kennedy, 1966, 1967; Studdert-Kennedy & Shankweiler, 1970).
As is generally well known, within the neocortical surface of the left hemisphere there is one area that largely controls the capacity to speak, and another region that mediates the ability to understand speech (Frost, et al., 1999; Goodglass & Kaplan, 1999; Heiss, et al., 1999; Pujol, et al., 1999). Specifically, Broca's expressive speech area is located along the left frontal convexity, whereas Wernicke's receptive speech area is found within the superior temporal lobe and becomes coextensive with the inferior parietal lobule.
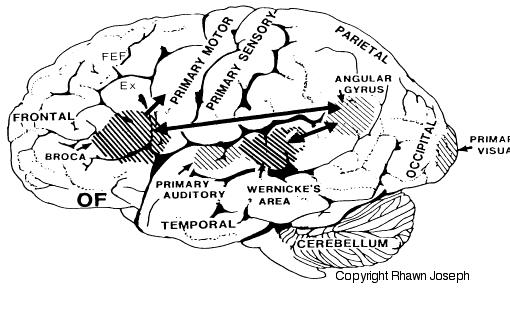
If Broca's area were severely damaged, the ability to speak would become severely impaired, although the patient would still be able to sing, swear and pray--singing, swearing and praying being mediated by the undamaged right hemisphere.
If Wernicke's receptive speech area were damaged, the ability to comprehend spoken and written language would be abolished.
Linking Broca's with Wernicke's area is the inferior parietal lobule and a thick band of fibers: the arcuate fasciculus. These areas interact to form a "language axis" and subserve those aspects of consciousness associated with language and thinking in words. The left hemisphere, therefore, is associated with what has classically been referred to as the conscious mind --though it must be stressed that this relationship only refers to those aspects of consciousness dependent on words and language.
THE RIGHT HEMISPHERE & UNCONSCIOUS SOCIAL EMOTONAL AWARENESS
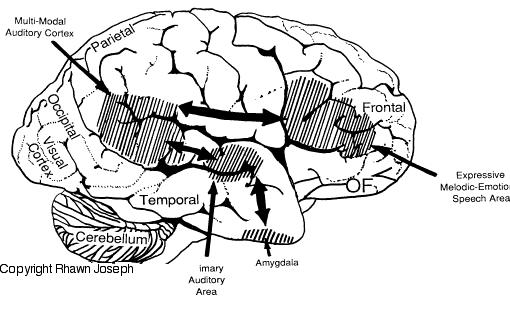
The right cerebral hemisphere is associated with visual spatial, non-verbal and emotional aspects of conscious awareness, including the emotional aspects of language and memory. That is, whereas the left hemisphere speaks and comprehends words and sentences and stores verbal memories, the right hemisphere vocalizes and comprehends emotional and melodic sounds and stores and recalls visual and emotional memories.
Hence, if someone were to say: "Do you want to go outside?" although the left hemisphere can speak and comprehend the words spoken, it is the right hemsphere which determines what the sentence means: If, for example, you are being threatened with a punch in the nose.
Hence, just as the left frontal and left regions mediates the expression and comprehension of the denotative aspects of speech, tissues in the right frontal and right temporal lobe mediates the expression and reception of the emotional and melodic aspects of speech; and these areas are interconnected by the corpus callosum.
Likewise, the right hemisphere stores and recall social emotional memories, (Cimino et al., 1991; Nunn et al., 1999; Ploner et al., 1999), and in fact demonstrates an increase in activity when recalling traumatic or depressing memories (Rauch et al., 1996, Shin et al., 1997; Abrams & Taylor, 1979; Cohen, Penick & Tarter, 1974; Deglin & Nikolaenko, 1975; Shagass et al.,1979).
The right hemisphere is in fact dominant in the perception, expression and mediation of almost all aspects of emotionality (Borod, 1992; Cimino et al., 1991; Joseph, 1982, 1986, 1988ab; Ross, 1993), including emotional vocalization and comprehension (Lalande et al. 1992; Ross, 1981; Shapiro & Danly, 1985; Tucker et al., 1977), as well as emotional memory.
This emotional dominance extends to bilateral control over the autonomic nervous system, including heart rate, blood pressure regulation, galvanic skin conductance and the secretion of cortisol in emotionally upsetting or exciting situations (Rosen et al. 1982; Wittling, 1990; Wittling & Pfluger, 1990; Yamour et al. 1980; Zamarini et al. 1990).
In part, it is believed that the right hemisphere dominance over emotional functioning is due to more extensive interconnections with the limbic system (Joseph, 1982, 1988a). The limbic system, in fact, appears to be functionally and structurally lateralized. For example, the appear to be more axonal connections between the neocortex of the right hemisphere and subcortical structures as the white matter connections are more extensive. The neocortex of the right hemisphere is also about 4% greater in size as compared to the left, the right amygdala is significantly (9%) larger than the left (Caviness, et al., 1997), whereas the left amygdala contains heavier concentrations of dopamine (Bradbury, Costall, Domeney, & Naylor, 1985; Stevens, 1992).
As originally proposed by Joseph (1982), over the course of evolution and development, limbic social-emotional functions have come to be hierarchically subserved by the right cerebrum due in part to the initial earlier maturation of the non-motor portions of the right cerebral neocortex and due to limbic laterality (Joseph, 1982, 1988a).
Thus, the right hemisphere has also come to dominate and to hierarchically process and express the purely emotional aspects of language, i.e. limbic language, which is why the right cerebrum is also dominate in regard to the expression and comprehension of emotional speech.
RIGHT HEMISPHERE MENTAL FUNCTIONING: THE UNCONSCIOUS MIND
That both halves of the brain are capable of supporting to independent mental domains, and that the right and left hemisphere subserve distinct realms of conscious awareness has been well demonstrated. This is evident in every day life, and is most dramatically evident when the axonal pathways linking the right and left hemisphere have been surgically destroyed. That is, the mental systems of the right and left hemisphere will begin to act independently and not always cooperatively.
As described by Nobel Lauriate Roger Sperry (1966, p. 299), "Everything we have seen indicates that the surgery has left these people with two separate minds, that is, two separate spheres of consciousness. What is experienced in the right hemisphere seems to lie entirely outside the realm of awareness of the left hemisphere. This mental division has been demonstrated in regard to perception, cognition, volition, learning and memory."
For example, when split-brain patients are tactually stimulated on the left side of the body, their left hemispheres demonstrate marked neglect when verbal responses are required, they are unable to name objects placed in the left hand, and they fail to report the presence of a moving or stationary stimulus in the left half of their visual fields (Bogen, 1979; Gazzaniga & LeDoux, 1978; Joseph, 1988b; Levy, 1974, 1983; Seymour et al. 1994; Sperry, 1982). They (i.e., their left hemisphere's) cannot verbally describe odors, pictures or auditory stimuli tachistoscopically or dichotically presented to the right cerebrum, and have extreme difficulty explaining why the left half of their bodies responds or behaves in a particular purposeful manner (such as when the right brain is selectively given a command).
In addition, they demonstrate marked difficulties in naming incomplete figures (and thus forming visual closure), as well as a reduced ability to name and identify nonlinguistic and environmental sounds (Joseph, 1986b, 1988b)--capacities associated with the functional integrity of the right hemisphere.
However, by raising their left hand (which is controlled by the right half of the cerebrum) the disconnected right hemisphere is able to indicate when the patient is tactually or visually stimulated on the left side. When tachistoscopically presented with words to the left of visual midline, although unable to name them, when offered mutiple visual choices in full field their right hemispheres are usually able to point correctly with the left hand to the word viewed.
In this regard, when presented with words like "toothbrush", such that the word "tooth" falls in the left visual field (and thus, is transmitted to the right cerebrum) and the word "brush" falls in the right field (and goes to the left hemisphere), when offered the opportunity to point to several words (i.e., hair, tooth, coat, brush, etc.), the left hand usually will point to the word viewed by the right cerebrum (i.e., tooth) and the right hand to the word viewed by the left hemisphere (i.e., brush). When offered a verbal choice, the speaking (usually the left) hemisphere will respond "brush" and will deny seeing the word "tooth."
Overall, this indicates that the disconnected right and left cerebral hemispheres, although unable to communicate and directly share information, are nevertheless fully capable of independently generating and supporting mental activity (Bogen, 1969, 1979; Gazzaniga & LeDoux, 1978; Joseph, 1986b, 1988b; Levy, 1974, 1983; Sperry, 1982). Hence, in the right hemisphere we deal with a second form of awareness that accompanies in parallel what appears to be the "dominant" temporal-sequential, language dependent stream of consciousness in the left cerebrum.
Moreover, as has been demonstrated by Joseph, Sperry, Bogen, Levy, and colleagues, the isolated right cerebral hemisphere, like the left, is capable of self-awareness, can plan for the future, has goals and aspirations, likes and dislikes, social and political awareness, can purposefully initiate behavior, guide responses choices and emotional reactions, as well as recall and act upon certain desires, impulses situations or environmental events --without the aid, knowledge or active (reflective) participation of the left half of the brain.
RIGHT BRAIN PERVERSITY
In that the brain of the normal as well as "split-brain" patient maintains the neuroanatomy to support the presence of two psychic realms, it is surprising that a considerable degree of conflict does not arise during the course of everyday activity. Frequently (such as in the case of the "split-brain" patient, LB, described below), although isolated the right half of the brain is fully willing to assist the left in a myriad of activities. Presumably such difficulties do not occur because both minds, having once been joined, share the same goals and interests. However, common experience seems to argue otherwise, for even in the intact individual, psychic functioning often is plagued by conflict.
In its most subtle manifestations the disconnected right hemisphere may attempt to provide the left with clues when the left (speaking) hemisphere is called upon to describe or guess what type of stimulus has been secretly shown to the right (such as in a T-scope experiment). Because the corpus callosum has been severed transfer and information exchange is not otherwise possible. Hene, when a picture has been shown to the right and the left has been asked to guess, the right hemisphere may listen and then nod the head or clear the throat so as to give clues or indicate to the left cerebrum that it has guessed incorrectly. In one case the right hemisphere attempted to trace or write an answer on the back of the right hand (e.g. Sperry et al. 1979). For example, after the right hemisphere was selectively shown a picture of Hitler, and then asked to indicate their attitude toward it before verbally describing it, the patient signalled "thumbs down".
EX: "That's another 'thumbs-down'?"
LB: "Guess I'm antisocial."
EX: "Who is it?"
LB: "GI came to mind, I mean..." Subject at this point was seen to be tracing letters with the first finger of the left hand on the back of his right hand.
EX: "You're writing with your left hand; let's keep the cues out."
LB: "Sorry about that."
Nevertheless, the behavior of the right hemisphere is not always cooperative, and sometimes it engages in behavior which the left cerebrum finds objectionable, embarrassing, puzzling, mysterious, and/or quite frustrating. This is probably true for the normal as well as the "split-brain" individual.
For example, Akelaitis (1945, p. 597) describes two patients with complete corpus callosotomies who experienced extreme difficulties making the two halves of their bodies cooperate. "In tasks requiring bimanual activity the left hand would frequently perform oppositely to what she desired to do with the right hand. For example, she would be putting on clothes with her right and pulling them off with her left, opening a door or drawer with her right hand and simultaneously pushing it shut with the left. These uncontrollable acts made her increasingly irritated and depressed."
Another patient experienced difficulty while shopping, the right hand would place something in the cart and the left hand would put it right back again. Both patients frequently experienced other difficulties as well . "I want to walk forward but something makes me go backward. ' A recently divorced male patient noted that on several occasions while walking about town he found himself forced to go some distance in another direction. Later (although his left hemisphere was not conscious of it at the time) it was discovered (by Dr. Akelaitis) that this diverted course, if continued, would have led him to his former wife's new home.
Geschwind (1981) reports a callosal patient who complained that his left hand on several occasions suddenly struck his wife--much to the embarrassment of his left (speaking) hemisphere. In another case, a patient's left hand attempted to choke the patient himself and had to be wrestled away (Goldstein; cited by Geschwind, 1981). Brion and Jedynak (cited by Geschwind, 1981) indicate that this type of independent left sided (right hemisphere) activity was common in their split-brain patients and termined it the "alien hand."
In addition, Bogen (1979, p. 333) indicates that almost all of his "complete commissurotomy patients manifested some degree of intermanual conflict in the early postoperative period." One patient, Rocky, experienced situations in which his hands were uncooperative; the right would button up a shirt and the left would follow right behind and undo the buttons. For years, he complained of difficulty getting his left leg to go in the direction he (or rather his left hemisphere) desired. Another patient often referred to the left half of her body as "my little sister" when she was complaining of its peculiar and independent actions.
A split-brain patient described by Dimond (1980, p. 434) reported that once when she had overslept her "left hand slapped me awake." This same patient, in fact, complained of several instances where her left hand had acted violently. Similarly, Sweet (1945) describes a female patient whose left hand sometimes behaved oppositionally and in a fashion which on occasion was quite embarrassing.
Similar difficulties plagued a split-brain patient on whom I reported on (Joseph 1988b). Indeed, after callosotomy, this patient (2-C) frequently was confronted with situations in which his left extremities not only acted independently, but engaged in purposeful and complex behaviors --some of which he (or rather, his left hemisphere) found objectionable and annoying.
For example, 2-C complained of instances in which his left hand would perform socially inappropriate actions (e.g. attempting to strike a relative) and would act in a manner completely opposite to what he expressively intended, such as turn off the TV or change channels, even though he (or rather his left hemisphere) was enjoying the program. Once, after he had retrieved something from the refrigerator with his right hand, his left took the food, put it back on the shelf and retrieved a completely different item "Even though that's not what I wanted to eat!" On at least one occasion, his left leg refused to continue "going for a walk" and would only allow him to return home.
In the laboratory, he often became quite angry with his left hand, he struck it and expressed hate for it. Several times, his left and right hands were observed to engage in actual physical struggles. For example, on one task both hands were stimulated simultaneously (while out of view) with either the same or two different textured materials (e.g., sandpaper to the right, velvet to the left), and the patient was required to point (with the left and right hands simultaneously) to an array of fabrics that were hanging in view on the left and right of the testing apparatus. However, at no time was he informed that two different fabrics were being applied.
After stimulation the patient would pull his hands out from inside the apparatus and point with the left to the fabric felt by the left and with the right to the fabric felt by the right.
Surprisingly, although his left hand (right hemisphere) responded correctly, his left hemisphere vocalized: "Thats wrong!" Repeatedly he reached over with his right hand and tried to force his left extremity to point to the fabric experienced by the right (although the left hand responded correctly! His left hemisphere didn't know this, however.). His left hand refused to be moved and physically resisted being forced to point at anything different. In one instance a physical struggle ensued, the right grappling with the left.
Moreover, while 2-C was performing this (and other tasks), his left hemisphere made statements such as: "I hate this hand" or "This is so frustrating" and would strike his left hand with his right or punch his left arm. In these instances there could be little doubt that his right hemisphere was behaving with purposeful intent and understanding, whereas his left brain had absolutely no comprehension of why his left hand (right hemisphere) was behaving in this manner.
LATERALIZED GOALS AND ATTITUDES
Why the right and left cerebral hemispheres in some situations behave cooperatively and yet in others in an oppositional fashion is in part a function of functional lateralization and specialization and the differential representation of social-emotional analytical abilities predominantly within the right hemisphere. Hence, because each hemisphere is concerned with different types of information, even when analyzing ostensibly the same stimulus may react, interpret and process it differently and even reach different conclusions (Joseph, 1988b; Levy & Trevarthen, 1976). Moreover, even when the goals are the same, the two halves of the brain may produce and attempt to act on different strategies.
Functional lateralization may thus lead to the development of oppositional attitudes, goals and interests. For example, one split brain individual's left hand would not allow him to smoke, and would pluck lit cigarettes from his mouth or right hand and put them out. Apparently, although his left ceebrum wanted to smoke, his right hemisphere didn't approve -apparently he had been trying to quite for years.
As noted above, 2-C experienced conflicts when attempting to eat, watch TV, or go for walks, his right and left brain apparently enjoying different TV programs or types of food (Joseph 1988b). Nevertheless, these difficulties are not limited to split-brain patients, for conflicts of a similar nature often plague the intact individual as well.
UNCONSCIOUS MEMORY FUNCTIONING
Although a variety of neurochemical and neuroanatomical regions are involved in the formulation of memory (Brewer et al., 1998; Gloor, 1997; Graff-Radford et al.1990; Halgren, 1992; Murray, 1992; Rolls, 1992; Sarter & Markovitch, 1985; Squire, 1992; Wagner et al., 1998; Victor et al 1989), functional specialization greatly determines what type of material can be memorized or even recognized by each half of the cerebrum. This is because the code or form in which a stimulus is represented in the brain and memory is largely determined by the manner in which it is processed and the transformations that take place.
Because the right and left cerebral hemispheres differentially process information, the manner in which this information is represented also will be lateralized (Bradshaw & Mattingly, 1997). Hence, some types of information only can be processed or stored by the right vs. the left cerebrum.
For example, it is well known that the left hemisphere is responsible for the encoding and recall of verbal memories, whereas the right cerebrum is dominant in regard to visual-spatial, non-verbal, and emotional memory functioning (Barr, Goldberg, Wasserstein & Novelly 1990; Brewer et al., 1998; Fried et al. 1982; Frisk & Milner 1990; Hecaen & Albert, 1978; Kimura, 1963. Levy, 1983; Milner, 1962, 1968; Nunn et al., 1999; Sperry et al., 1979; Squire, 1992; Suberi & McKever, 1977; Wechsler, 1973; Whitehouse, 1981). If the left temporal lobe were destroyed, verbal memory functioning would become impaired since the right cerebrum does not readily store this type of information. Conversely, the left has great difficulty storing or remembering nonlinguistic, visual, spatial, and emotional information.
Specifically, left temporal lobectomy, seizures or lesions involving the inferior temporal areas can moderately disrupt immediate and severely impair delayed memory for verbal passages, and the recall of verbal paired-associates, consonant trigrams, word lists, number sequences, and conversations (Barr et al. 1990; Delaney et al. 1980; Kapur et al. 1992; Meyer & Yates,1955; Milner 1968; Milner & Teuber 1968; Samson & Zatorre, 1992; Weingartner 1968). Similarly, severe anterograde and retrograde memory loss for verbal material has been noted when the left anterior and posterior temporal regions (respectively) are electrically stimulated (Ojemann et al. 1968, 1971), lobectomized or injured (Barr et al. 1990; Kapur et al. 1992).
In contrast, right temporal lesions or lobectomy significantly impairs recognition memory for tactile and recurring visual stimuli such as faces and meaningless designs, memory for object position and orientation, and visual-pictorial stimuli, and short-term memory for melodies (Corkin 1965; Delaney et al. 1980; Kimura 1963; Milner 1968; Nunn et al., 1999; Ploner et al., 1999; Samson & Zatorre, 1988, 1992; Taylor 1979). Similarly, memory for emotional material is also significantly impaired with right vs left cerebral lesions (Cimino et al. 1991; Wechsler 1973) including the ability to recall or recognize emotional faces (DeKosky, et al. 1980; Fried et al. 1982; Weddell, 1989). Individuals with right hemisphere damage also have more difficulty recalling personal emotional memories (Cimino et al. 1991).
Hence, it is the left hemisphere which is responsible for the encoding and recall of verbal, temporal-sequential, and language related memories, whereas the right cerebrum is dominant in regard to visual-spatial, non-verbal, and social emotional memory functioning. Each hemisphere stores the type of material that it is best at recognizing, processing, and expressing.
UNILATERAL (UNCONSCIOUS) MEMORY STORAGE
In the intact, normal brain, even non-emotional memory traces appear to be stored unilaterally rather than laid down in both hemispheres (Bures & Buresova 1960; Doty & Overman 1977; Hasegawa et al., 1998; Kucharski et al. 1990; Levy, 1974; Risse & Gazzaniga, 1979). Moreover when one hemisphere learns, has certain experiences, and/or stores information in memory, this information is not always available to the opposing hemisphere; one hemisphere cannot always gain access to memories stored in the other half of the brain (Bures & Buresova 1960; Doty & Overman 1977; Hasegawa et al., 1998; Joseph, 1986b, 1988ab, 1992b; Kucharski et al. 1990; Levy, 1974; Risse & Gazzaniga 1979).
To gain access to these lateralized memories, one hemisphere has to activate the memory banks of the other brain half via the corpus callosum (Doty & Overman, 1977; Hasegawa et al., 1998) or anterior commissure (Kucharski et al. 1990). This has been demonstrated experimentally in primates. For example, after one hemisphere had been trained to perform a certain task, although either hemisphere could respond correctly once it was learned, when the commissures were subsequently cut, only the hemisphere that originally was trained was able to perform--i.e., could recall it. The untrained hemisphere acted as though it never had been exposed to the task; its ability to retrieve the original memories was now abolished (Doty & Overman, 1977; see also Hasegawa et al., 1998).
In a conceptually similar study, Risse and Gazzaniga (1979) injected sodium amytal into the left carotid arteries of intact patients so as to anesthetize the left cerebral hemisphere. After the left cerebrum was inactivated, the awake right hemisphere, although unable to speak, was still able to follow and behaviorally respond to commands, e.g., palpating an object with the left hand.
Once the left hemisphere had recovered from the drug, as determined by the return of speech and motor functioning, none of the eight patients studied was able to verbally recall what objects had been palpated with the left hand, "even after considerable probing." Although encouraged to guess most patients refused to try and insisted that they did not remember anything. However, when offered multiple choices in full field, most patients immediately raised the left hand and pointed to the correct object!
According to Risse and Gazzaniga (1979), although the memory of touching and palpating the object was not accessible to the verbal (left hemisphere) memory system, it was encoded in a nonverbal form within the right hemisphere and was unavailable to the left hemisphere when normal function returned. The left (speaking) hemisphere was unable to gain access to information and memories stored within the right half of the brain. Nevertheless, the right brain not only remembered, but was able to act on its memories.
This indicates that when exchange and transfer is not possible, is in some manner inhibited, or if for any reason the two halves of the brain become functionally disconnected and are unable to share information, the possibility of information transfer at a later time is precluded (Bures & Buresova, 1960; Hasegawa et al., 1998; Kucharski et al. 1990; Risse & Gazzaniga, 1979) -even when the ability to transfer is acquired or restored. The information is lost to the opposite half of the cerebrum.
Moreover, because some types of information are processed by the right and left hemisphere in a wholly different fashion, they are unable to completely share or gain access to the data or even the conclusions reached by the other -as they are unable to process or recognize it -which in turn precludes complete interhemispheric transfer (Berlucchi & Rizzolatti, 1968; Hicks, 1974; Joseph, 1982, 1988a; Marzi, 1986; Merriam & Gardner, 1987; Miller, 1990, 1991; Myers, 1959, 1962; Rizzolatti et al. 1971; Taylor & Heilman 1980); information is lost during the transfer process.
Nevertheless, although inaccessible or lost, these memories, details, and attached feelings can continue to influence whole brain functioning in subtle as well as in profound ways. That is, one hemisphere may experience and store certain information in memory and at a later time in response to certain situations act on those memories, much to the surprise, perplexity, or chagrin of the other half of the brain; one hemisphere cannot always gain access to memories stored in the other half of the brain.
Dreaming.
Of course, complete functional deactivation is probably quite rare in the normal brain. However, there is some evidence to suggest that interhemispheric communication is reduced, for example, during sleep and possibly during dreaming (Banquet, 1983; Joseph, 1988a).
Most dreaming occurs during REM, which possibly is associated with right hemisphere activation and low-level left hemisphere arousal (Goldstein et al. 1972; Hodoba, 1986; Meyer et al. 1987). It also becomes progressively more difficult to recall one's dreams as one spends time in or awakens during NonREM (Wolpert & Trosman, 1958), which is associated with high left hemisphere and low right brain activation (Goldstein et al. 1972). Thus are dreams really forgotten, or are they locked away in a code which is not accessible to the speaking left hemisphere?
DREAMS & EMOTIONAL TRAUMA
Given right cerebral dominance for emotion and dream production, it is perhaps not surprising that emotional conflicts and traumas are often represented via dream imagery (Freud, 1900, Joseph, 1992b; Jung, 1945).
Consider, for example, Sara, who was desribed by her parents as a "very good and obedient" 6 year old girl who suffered from "night terrors" (Joseph, 1992b). Specifically, she frequently woke up at night screaming about the "creek," that ran near her home. According to her mother, Sara was afraid because she had been told that hoboes lived under the bridge and to never go there without her mommy or daddy, because they would "get" her.
I had Sara tell me her dream.
Sara: "I'm walking on the sidewalk near the big creek. Then I go to the edge and stare down at the big rocks at the bottom. All at once the whole world starts to shake. Like it's turning upside down. It's trying to throw me into the creek. I get scared and start to be afraid and start grabbing at the trees and bushes to keep from falling into the creek and onto the big rocks. Sometimes I see this hole and I crawl in. Then everything is OK. Sometimes I fall and fall and fall and I can see the big rocks coming closer and I know I'm going to fall on them. When I fall on them I wake up 'cause it hurts."
Sara had this particular dream repeatedly. Was it really because she was afraid of the hoboes and the creek?
In Sara's case it is noteworthy that her parents fought, screamed, yelled, and argued almost non-stop and there were constant threats of divorce. From talking within Sara it was also apparent that she was traumatized by her parents constant fighting -although they were both ostensibly quite good to her. Nevertheless, Sara's world was being turned up side down and was in complete chaos, which was reflected in her dreams.
Sara also had another troubling and recurrent dream where she went riding on her bike and when she came back to her street, her house was gone. Every house on the street was the same, including the neighbors. But when she asked about her family, no one knew what she was talking about and no one recognized her.
Although the symbolic content of these dreams was not apparent to Sara or her mother, one need not be a psychiatrist to decipher their obvious meaning. Sara's emotional world was literally being turned upside down and was in chaos due to the horrible fighting engaged in by her parents. She was terrified of losing her home and the catastrophe she perceived as befalling her family. Her very identity and functional integrity as a person was at stake, for if she lost her family she lost her Self.
The dream imagery involving the hole that she climbs into is also very interesting in that it suggests the desire to return to the safety and security of the womb. On the other hand, the hole" may have been exactly that, a hole. Indeed, dreams frequently mean exactly what they seem to mean (Jung, 1945).
Nevertheless, it might reasonably be asked, if dreams are of importance and not merely reflective of random and purely confabulatory ideation, why are they so difficult to recall? In part, as noted in the introduction to this section, this may be a function of lateralization, alterations in hemispheric arousal and activity, differential memory storage, and decreased interhemispheric communication during REM. Perhaps they only can be recalled by the right hemisphere. Of course, in some instances, dreams are probably nothing more than mundane and confabulatory noise.
LONG LOST CHILDHOOD MEMORIES
For most individuals it is extremely difficult if not impossible to verbally recall events which occurred before the age of three and a half (Dudycha & Dudycha, 1933; Gordon, 1928; Joseph, 2000; Waldvogel, 1948; White & Pillemer,1979). . There are several reasons for this (see chapter 29).
Information processed and experienced during infancy vs. adulthood is stored via certain transformations and retrieval strategies which are quite different. As the brain matures and new information processing strategies are learned and developed, the manner in which information is processed and stored is altered. Although these early memories are stored within the brain, the organism no longer has the means of retrieving them, i.e., the key no longer fits the lock.
That is, early experiences may be unrecallable because infants use a different system of codes to store memories whereas adults use symbols and associations (such as language) not yet fully available to the child (Dollard & Miller, 1950; Joseph, 1982, 2000; Piaget, 1952, 1962, 1974). Much of what was experienced and committed to memory during early childhood took place prior to the development of lingusitic labeling ability and was based on a pre- or nonlinguistic code (Dollard & Miller, 1950; Freud, 1900). Hence, the adult, who is relying on more sophisticated and language-related coding systems, cannot find the right set of neural programs to open the door to childhood memories. The key does not fit the lock because the key and the lock have changed.
The inability to recall early memories is also a function of programmed cell death--the loss of memory-laden neurons which are shed by the millions over the course of early development and the immaturity of the corpus callosum in children (Joseph, 1999b, 2000). That is, non-verbal information perceived and processed by the right vs left hemisphere is generally stored in the right vs left hemisphere. Later, when the commissures mature, this information cannot be transferred except under special conditions.
However, under conditions of traumatic memory loss; e.g. repression, not just the the right and left hemisphere, but the differential activation of and injury to the amygdala and hippocampus are contributory; and later the recall of such memories may be opposed by the frontal lobes; the right frontal in particular (Joseph, 1982, 1986, 1988, 1990, 1996, 1999, 2000)
EMOTION AND RIGHT BRAIN FUNCTIONING IN CHIDLREN
As is now well known, the developing organism is extremely vulnerable to early experience during infancy such that the nervous system, perceptual functioning and behavior may be altered dramatically (Bowlby 1982; Casagrande & Joseph 1978; 1980; Diamond, 1985, 1991; Denenberg 1981; Ecknerode et al. 1993; Harlow & Harlow 1965; Joseph 1979; Joseph & Casagrande 1980; Joseph & Gallagher 1980; Joseph et al. 1978; Langmeier & Matejcek 1975; Rosenzweig 1971; Salzinger et al.1993; Sternberg et al. 1993). Interestingly, there is some evidence that the right cerebral hemisphere and the right amygdala may be more greatly affected (see Denenberg 1981; Diamond, 1985).
Moreover during these same early years our traumas, fears, and other emotional experiences, like those of an adult, are mediated not only by the limbic system, but also via the nonlinguistic, social-emotional right hemisphere. And, just as they are in adulthood, these experiences are stored in the memory banks of the right cerebrum.
However, much of what was experienced and learned by the right half of the brain during these early years was not always shared or available for left hemisphere scrutiny (and vice-versa). That is, a childs two hemispheres are not only functionally lateralized, but limited in their ability to share and transfer information. In many ways, infants and young children have split-brains (Deruelle & de Schonen, 1991; Finlayson 1975; Gallagher & Joseph 1982; Galin et al. 1979ab; Joseph & Gallagher, 1985; Joseph et al. 1984; Kraft et al. 1980; Molfese et al. 1975; O'Leary 1980; Ramaeker & Njiokiktjien, 1991; Salamy 1978; Yakovlev & Lecours 1967).
Indeed, due to the immaturity of the corpus callosum and in particular, the slow rate of axonal myelin within the callosum (Yakovlev & Lecours, 1967), communication is so poor that children as old as age 4 have mild difficulty transfering tactile, auditory, or visual information between the hemispheres, e.g., accurately describing complex pictures shown to the right brain (Joseph et al. 1984). That is, in addition to differential functional specialization, the slow development of the myelination process can in turn slow and disrupt axonal information transmission (e.g. Konner, 1991; Ritchie, 1984; Salamy 1978).
Indeed, although pain can be transmitted and received via axons devoid of myelin, this type of data is completely lacking in complexity and is devoid of initial cognitive attributes. Pain transmitting axons have very simple requirements. By contrast as data complexity increases, so too does the complexity of those neurons which transmit these signals (Konner, 1991; Ritchie, 1984).
For example, as axon diameter increases, so too does the extent of myelination. Similarly, quantities of axoplasm and cytoplasm, nuclear diameter, and neuronal packing density are also correlated with myelination (Konner, 1991). Conversely, lack of myelin, or those neurons which have not yet myelinated, are associated with an increased susceptibility to conduction failure and interference due extraneous influences, including signal modification by neighboring axons (Konner, 1991; Ritchie, 1984).
FUNCTIONAL COMMISSUROTOMIES AND LIMITIED INTERHEMISPHERIC TRANSFER
The corpus callosum is the gateway via which information may travel from one brain half to the other. However, it also acts to limit information exchange since almost 40% of the adult callosum lacks myelin (Selnes, 1974). Since mylein acts to insulate and, thus, preserve information transmission by minimizing leakage and increasingly conduction velocity and integrity (Konner, 1991; Rogart & Ritchi, 1977; Ritchie, 1984), some information is lost and degraded even when transfer is possible. (Berlucchi & Rizzolatti, 1968; Hicks 1974; Joseph et al. 1984; Marzi, 1986; Merriam & Gardner, 1987; Myers, 1959, 1962; Rizzolatti et al. 1971; Taylor & Heilman 1980).
Moreover, particularly when one is dealing with complex or emotional information situations probably sometimes arise in which one brain half has little or no knowledge as to what is occurring in the other (Dimond, 1980; Dimond & Beaumont, 1974; Dimond et al. 1972; Geschwind, 1965; Joseph, 1982, 1988a, 1992b; Joseph et al. 1984; Marzi, 1986; Myers, 1959). In part, this is a consequence of lateralized specialization. Certain forms of information can only be processed and, thus, recognized by the right or left half of the brain. Even information that is transferred may be subject to interpretation and miss-interpretation (Joseph, 1982, 1986ab, 1988ab; Joseph et al., 1984) and this includes even the learning of sequential and fine motor movements (Hicks 1974; Taylor & Heilman 1980; see also Parlow & Kinsbourne 1989).
In addition, one brain half can be prevented from knowing what is occurring in the opposite half due to inhibitory or suppressive actions initiated by, for example, the frontal lobes, such that certain forms of information are suppressed, censored, and inter-hemispheric (as well as intra-hemispheric) information transmission prevented (Hoppe, 1977; Joseph, 1982, 1988a, 1992b). Thus, there sometimes results a functional commissurotomy (Hoppe, 1977; see also Galin, 1974).
Therefore, these three conditions --lateralized specialization, frontal lobe inhibitory activity, and incomplete myelination of callosum axons-- can reduce the ability of the two hemispheres to communicate among normal, intact individuals. Hence, in many ways the brain of even a normal adult is functionally split and disconnected, and for good reason. These conditions protect the brain and linguistic consciousness from becoming overwhelmed. As we have seen with frontal lobe damage, when communication is allowed to occur freely (due to disinhibition) the overall integrity of the brain to function normally is curtailed dramatically.
Nevertheless, a unique side effect of having two brains that are not always able to communicate completely and successsfully is intra-psychic conflicts. That is, we sometimes find ourselves feeling happy, sad, depressed, angry, etc. without a clue as to the cause. In other instances, we actually may commit certain thoughtless, impulsive, overly emotional, or embarassing actions and "have no idea" as to "what came over" us. To posit the notion that we have such experiences simpl "because" is absurd. Nor, among "normals," are such experiences always due to biochemical fluctuations or the result of "unconscious" urges. Rather, unbeknownst to the left brain, sometimes the right perceives, remembers, or responds to some external or internal source of experience and/or to its own memories and, thus, reacts in an emotional manner. The left (speaking ) hemisphere in turn only knows that it is feeling something but is unsure what or why , or, conversely, confabulates various denials, rationalizations and explanations which it accepts as fact.
SPLIT-BRAIN FUNCTIONING IN CHILDREN: THE ONTOLOGY OF EMOTIONAL CONFLICT
Thus, due in part to the slow pace of corpus callosum myelination, coupled with differential right and left cerebral specialization, the left hemisphere of a young child has at best incomplete knowledge of the contents and activity that are occurring within the right. This sets the stage for differential memory storage and a later inability to transfer this information between the cerebral hemispheres once the child reaches adulthood.
Because of lateralization and limited exchange, the effects of early "socializing" experience can have potentially profund effects. "As a good deal of this early experience is likely to have unpleasant if not traumatic moments, it is fascinating to consider the later ramifications of early emotional learning occurring in the right hemisphere unbeknownst to the left; learning and associated emotional responding that later may be completely inaccessibile to the language centers of the left half of the brain. That is, although limited transfer in children confers advantages, it also provides for the eventual development of a number of very significant psychic conflicts --many of which do not become apparent until much later in life."
Moreover, due to the immaturity of the callosum, children frequently can encounter situations in which the right and left cerebrum not only differentially perceive what is going on, but are unable to link these experiences so as to understand fully what is occurring or to correct misperceptions (Galin, 1974; Joseph, 1982, 1992b). Consider, for example, a young divorced mother with ambivalent feelings toward her young son (Galin, 1974; Joseph, 1988a, 1992b).
Although she does not express these feelings verbally, she conveys them through her tone of voice, facial expression, and in the manner in which she touches her son. She knows that she should love him, and at some level she does. She wants to be a good mother and makes herself go through the motions. However, she also resents her son because she has lost her freedom, he is a financial burden, and he may hinder her in finding a desirable mate. She is confronted by two opposing attitudes, one of which is unacceptable to the image she has of a good mother. Like many of us, she must prevent these feelings from reaching linguistic consciousness. However, this does not prevent them from being expressed nonlingusitically via. the right brain.
Her son, of course, also has a right hemisphere which perceives her tension and amibivalance. The right half of his brain notes the stiffness when his mother holds or touches him and is aware of the manner in which she sometimes looks at him . Worse, when she says, "I love you," his right hemisphere senses the tension and tone of her voice and correctly perceives that what she means is, "I don't want you" or, "I hate you. " His left hemisphere hears, however, "I love you" and notes only that she is attentive. He is in a "double bind" conflict, with no way for his two cerebral hemispheres to match impressions.
The right half of this little boy's brain feels something painful when the words "I love you" are spoken. When his mother touches him, he becomes stiff and withdrawn because his right hemisphere, via the analysis of facial expression, emotional tone, tactile sensation, etc. is fully aware that she does not want him.
Later, as an adult, this same young man has one failed relationship after another. He feels that he can't trust women, often feels rejected, and when a girl or woman says "I love you," it makes him want to cringe, run away, or strike out. As an adult, his left hemisphere hears "Love," and his right cerebrum feels pain and rejection.
Because the two halves of his cerebrum were not in communication during early childhood, his ability to gain insight into the source of his problems is greatly restricted. The left half of his brain cannot access these memories. It has "no idea" as to the cause of his conflicts.
In this regard, this asymmetrical arrangement of hemispheric function and maturation may well predispose the developing child in later life to come upon situations in which it finds itself responding emotionally, nervously, anxiously, or neurotically, without linguistic knowledge, or without even the possiblity of linguistic comprehension as to the cause, purpose, eliciting stimulus, or origin of its behavior. As a child or an adult, it may find itself faced with behavior that is mysterious, embarrassing, etc. "I don't know what came over me."